Ohio Medicaid Sterilization Consent Form - (1) claims for sterilization and hysterectomy procedures must be submitted to. Complete all fields unless indicated as optional. The ohio department of medicaid (odm) has developed guidelines for completing. This form allows an individual to provide consent for sterilization. Effective april 1, 2018, medicaid providers must submit odm 03199. The consent for sterilization form is. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215.
Effective april 1, 2018, medicaid providers must submit odm 03199. The ohio department of medicaid (odm) has developed guidelines for completing. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. This form allows an individual to provide consent for sterilization. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. (1) claims for sterilization and hysterectomy procedures must be submitted to. The consent for sterilization form is. Complete all fields unless indicated as optional.
Effective april 1, 2018, medicaid providers must submit odm 03199. (1) claims for sterilization and hysterectomy procedures must be submitted to. Complete all fields unless indicated as optional. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. The ohio department of medicaid (odm) has developed guidelines for completing. This form allows an individual to provide consent for sterilization. The consent for sterilization form is.
Texas Medicaid Sterilization Consent Form 2019 2024 Printable Consent
(1) claims for sterilization and hysterectomy procedures must be submitted to. This form allows an individual to provide consent for sterilization. Complete all fields unless indicated as optional. Effective april 1, 2018, medicaid providers must submit odm 03199. The ohio department of medicaid (odm) has developed guidelines for completing.

Medicaid Consent Form For Sterilization 2023 Printable Consent Form 2022
Effective april 1, 2018, medicaid providers must submit odm 03199. This form allows an individual to provide consent for sterilization. Complete all fields unless indicated as optional. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215.
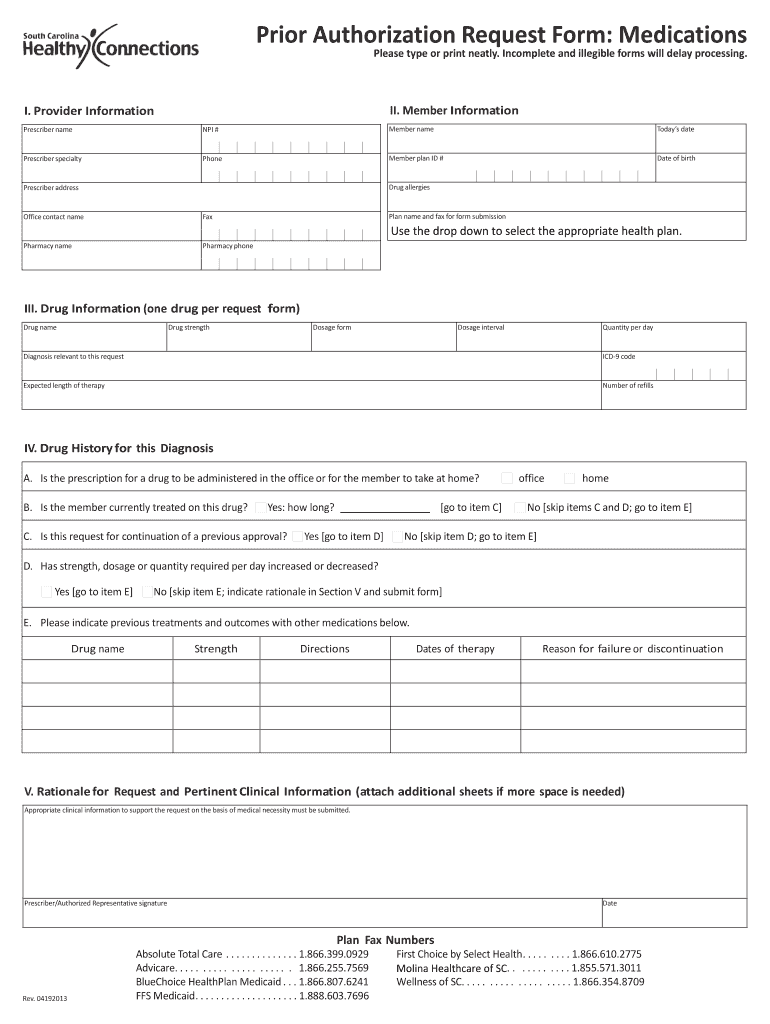
South Carolina Medicaid Sterilization Consent Form 2024 Printable
Complete all fields unless indicated as optional. Effective april 1, 2018, medicaid providers must submit odm 03199. The consent for sterilization form is. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. (1) claims for sterilization and hysterectomy procedures must be submitted to.

Florida Medicaid Sterilization Consent Form 2019 2023 Printable
Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. This form allows an individual to provide consent for sterilization. The consent for sterilization form is. Effective april 1, 2018, medicaid providers must submit odm 03199.

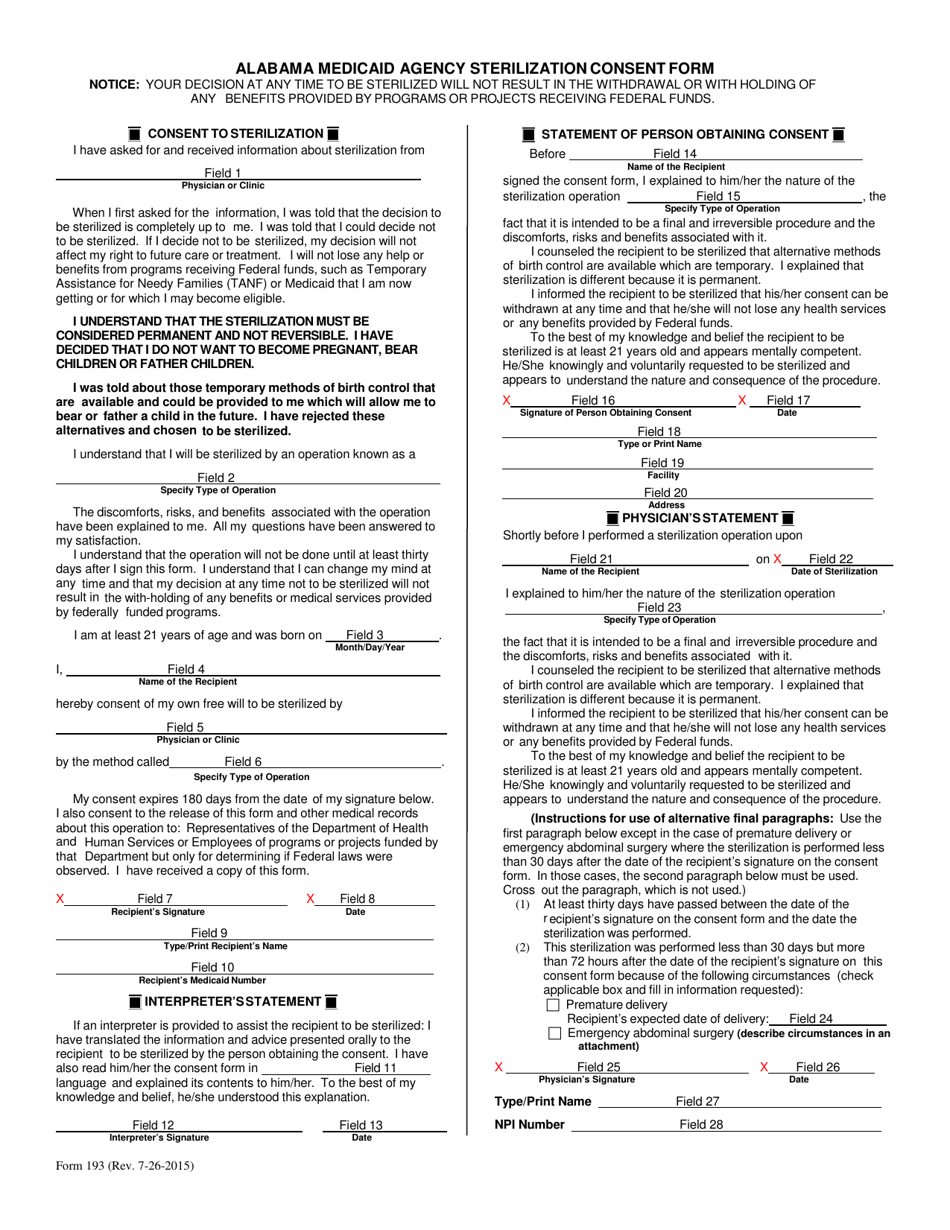
Informed Consent Form For Sterilization Operation PDF Medical
This form allows an individual to provide consent for sterilization. Effective april 1, 2018, medicaid providers must submit odm 03199. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. (1) claims for sterilization and hysterectomy procedures must be submitted to. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,.

Ohio Medicaid Sterilization Consent Form 2022 Printable Consent Form 2022
The consent for sterilization form is. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. The ohio department of medicaid (odm) has developed guidelines for completing. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. This form allows an individual to provide consent for sterilization.
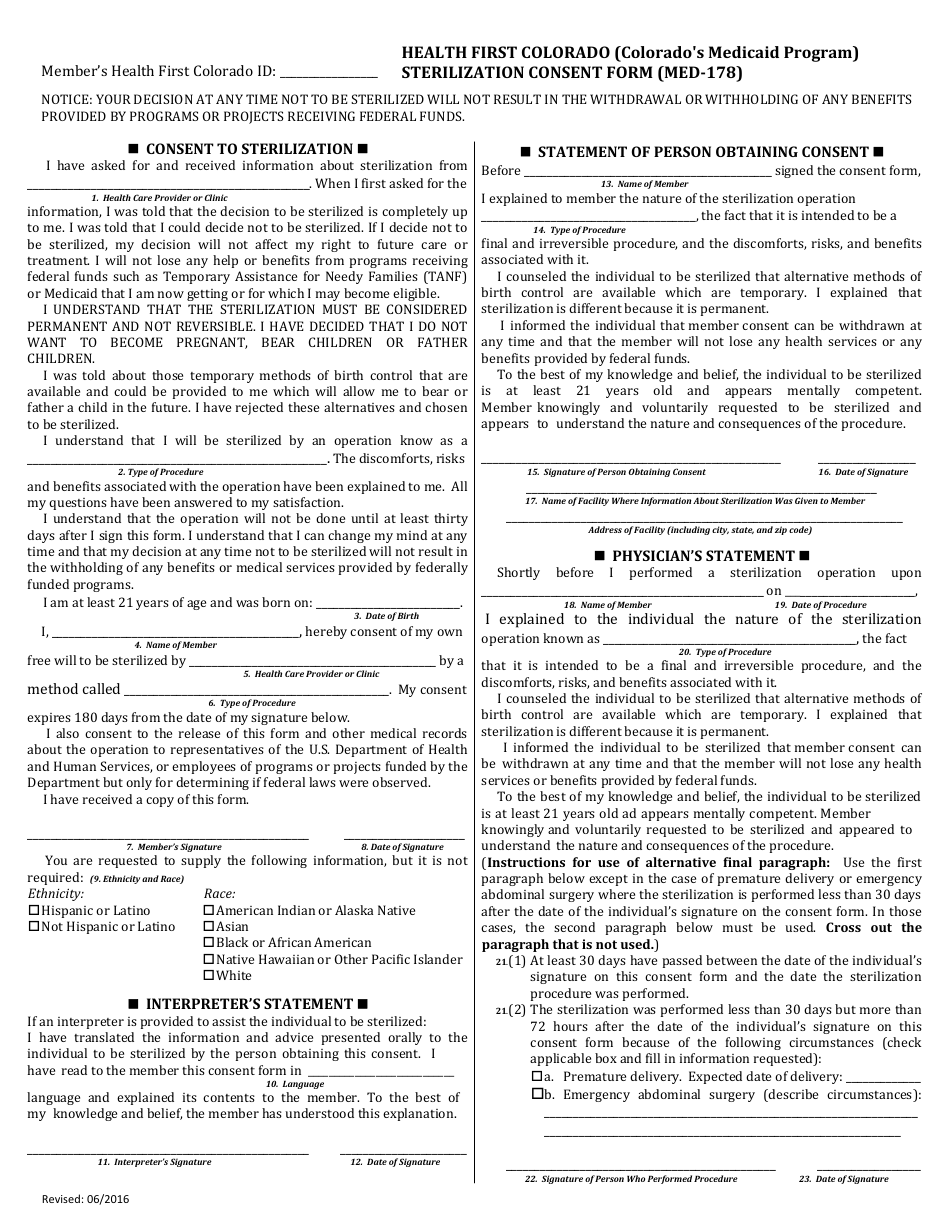
Form MED178 Fill Out, Sign Online and Download Printable PDF
Effective april 1, 2018, medicaid providers must submit odm 03199. (1) claims for sterilization and hysterectomy procedures must be submitted to. Complete all fields unless indicated as optional. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. This form allows an individual to provide consent for sterilization.

Hysterectomy Consent Form For Ohio Medicaid 2023 Printable Consent
The consent for sterilization form is. This form allows an individual to provide consent for sterilization. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. (1) claims for sterilization and hysterectomy procedures must be submitted to.

Pennsylvania Medicaid Sterilization Consent Form 2022 Printable
Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. The ohio department of medicaid (odm) has developed guidelines for completing. Complete all fields unless indicated as optional. This form allows an individual to provide consent for sterilization. The consent for sterilization form is.
Medicaid Sterilization Consent Form 2025 Diana Davidson
Complete all fields unless indicated as optional. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. The consent for sterilization form is. Effective april 1, 2018, medicaid providers must submit odm 03199. Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215.
The Consent For Sterilization Form Is.
Effective april 1, 2018, medicaid providers must submit odm 03199. (1) claims for sterilization and hysterectomy procedures must be submitted to. In accordance with title 42 code of federal regulations (cfr), part 441, subpart f,. The ohio department of medicaid (odm) has developed guidelines for completing.
Complete All Fields Unless Indicated As Optional.
Ohio department of medicaid | 50 west town street, suite 400, columbus, ohio 43215. This form allows an individual to provide consent for sterilization.